You can create your own holidays! On this page I share some of mine.
Backup DayJanuary 5th
Check your backup document which lists where all important data is stored
All important data should have at least one clearly-documented backup location (ideally two)
Consider automating your backups if they are not already
Consider if you have to back up anything physical (IDs, passports, tax documents, mail)
Make sure your backups actually work
Security Audit DayFebruary 5th
Upgrade all your computers, servers, firewalls, and packages
Do basic penetration testing, remove deprecated software
Delete accounts/info you don’t need, attempt to doxx yourself if you want more opsec
Briefly go over physical security with a reasonable threat model too (keys, cameras, etc are cheap)
Digital Organization DayMarch 5th
Organize and categorize all your files and directories on all your devices
Clean your desktop, home screen, task bar, delete unused apps
Physical Organization DayApril 5th
Organize and categorize all the objects in your living space
Buy anything that helps you become more organized such as cable ties, organizers, plastic bags, extension cables, label maker, etc
Don’t be averse to replacing old or sub-optimal items if you can afford newer ones – it’s usually worth it
Cancel Subscriptions DayMay 5th
Cancel or reduce as many reoccurring payments as possible
Check all credit cards, bank accounts, mortgage accounts, brokerage accounts, business accounts, etc and repeat this process
Consider the rest of your personal finances too, but you should do this more than once a year!
Habit Breaking DayJune 5th
Break as many habits as you can: stop yourself before you perform any habitual action and first attempt an alternative
You are not allowed to engage in a habit before at first consciously stopping to analyze at least one alternative (including simply not doing it) and performing a basic EV analysis
Try to apply this at a low level, e.g. including phone apps you open – It’s very hard!
You will probably want to modify your environment both physically (keep your phone further away) and digitally (block common websites) for a reasonably serious attempt
Cold Outreach DayJuly 5th
Do cold outbound!
If you don’t know anyone you want to talk to or meet, look for new people
Digital Exploration DayAugust 5th
The Internet is a large place and is not actually only composed of four apps
Explore it! Find places you’d never normally go to – links were made to be clicked!
You may naturally find yourself falling into Internet rabbit holes, but the intent of today is to dig new holes rather than fall into pre-existing patterns
Optionally pair with learning new skills, hobbies, or interacting with new types of people
Belief Audit DaySeptember 5th
Spend at least several hours auditing beliefs that you hold dear
Make a document and recursively lists beliefs you hold about the world and yourself with reasons for why
Then red-team the ideas and attempt to falsify them.
It’s likely that this is most difficult for beliefs which are harming you the most.
Suggested to be done entirely in written format, although walks are also acceptable for single topics
Health Analysis DayOctober 5th
Analyze your personal health data and think of new data you may want to collect
With generative AI you can code and parse data much more quickly than before. It took me 10 minutes to import apple health data into a custom sql database starting with nothing but Claude
Consider blood tests – you can order them yourself with services like privatemdlabs and it’s one of the best ways to find ways to improve yourself (your goal should not be to fall “within the range” but rather to be at optimal levels of useful biomarkers like hormones, A1C, CRP, Lp(a), homocysteine, triglycerides. If you’re taking a test that’s important to you, you don’t shoot for a 60 or 70, but instead a perfect score.
If you can find ways to spend money to improve your health, it’s probably worth it. It’s easy to have fun with data from an (apple watch, eight sleep, whoop, oura, cgm, dexascan), but make sure the product is actually what you need to improve yourself beforehand. Data is fun, but actionable data is even more fun!
$X Celebration DayNovember 5th
Today is the day to celebrate $X (this is a fill in-the-blank variable, not Twitter!), something which you love but for some reason the rest of humanity has not made a national holiday for
If you really love $X, you could make this a monthly celebration, or perhaps even…
Spread this holiday to as many people as possible if you’d like a shot at it becoming a real national holiday
Bespoke Holiday DayDecember 5th
Are your bespoke holidays helping?
Can you improve them or add new ones?
My original list had twice as many holidays, so I’m confident you can come up with more!
Celebrate these holidays with just a few clicks!
You can add all of the above holidays to your calendar with this link! Google calendar instructions: Open your calendar and find the bottom left hand panel where it says Other calendars. Click + and then from URL and paste in the above link.
Scott Alexander of SlateStarCodex / AstralCodexTen recently wrote Pascalian Medicine, in which he looks at various substances purported to improve covid outcomes, but which have relatively low amounts of evidence in their favor, likening administration of all of them to patients to a Pascal’s wager-type argument: if there is a small probability of a potential treatment helping with covid, and if it’s also very unlikely that this treatment is harmful, should we just give it to the patient regardless of if the quality of evidence is low and uncertain, as it would clearly have a positive expected outcome regardless?
The naive answer to this could simply be to attempt to calculate an expected value (note: I use the term expected value often here, but in some cases the terms hazard ratio, relative risk, or odds ratio would be more appropriate) for each treatment, and administer it if it’s positive. But there could be some unintended consequences of using this methodology over the entire set of potential treatments: we could end up suggesting treatments of 10 or 100+ pills for conditions, and apart from something just feeling off about this, it could magnify potential drug interactions, some treatments could oppose others directly, the financial cost could start to become prohibitive, and it could decrease patient confidence and have many other undesirable second-order effects.
Pascalian Longevity
There are many counter-arguments presented to the above concept which become less salient when the goal is changed from ‘find drug treatments to prescribe to all covid patients’ to ‘find personal health interventions that increase your own lifespan/longevity’.
I am fortunate enough that I am able to evaluate potential longevity interventions myself, pay for them myself, administer them myself, and review their potential effects on me myself. I might not do a perfect job of this – research is difficult, time-consuming, and lacking in rigor and quantity, and finding appropriate longevity biomarkers to quantitatively asses the effects of interventions is also difficult. But uncertainty is a given here, and that is why we incorporate it into our frameworks when deciding if something is worth doing or not by calculating an expected value. Furthermore, any harm that I may accidentally incur will only be done to myself, reducing the ethical qualms of this framework to near-zero (I would strongly oppose arguments that I should not have the right to take drugs which I think may significantly improve my own health, although some may disagree here).
My modus operandi with respect to longevity may have many uncertainties in its output, but still operates with a very strong (in my opinion) positive expected value: If a substance significantly and consistently increases the lifespan of organisms similar to humans (ideally in humans), and is also very safe in humans, then it is something that I want to take
This is how I operate personally with longevity, and it does result in me taking quite a few things (currently I’m at around 15). I do still try to minimize what I take as a meta-principle (for example, setting a minimum threshold of expected value that a substance must provide to warrant inclusion, rather than simply accepting any positive expected value) for a few reasons: firstly, to reduce potential drug interactions (which we do attempt to asses on a per-substance basis, rather than account for as an unknown, but unknowns are unfortunately a very large component of messing with biology regardless). Secondly, to keep my costs relatively sane, although I am not too worried about this as there are few ways to spend money more effectively than on trying to improve your health. Thirdly, to reduce the occurrence of interventions that may have the same or opposing mechanisms of action (taking two things with the same mechanism of action may be okay, but sometimes dose-response curves are less favorable, and taking >~2x of something will result in diminished or even negative returns). Lastly, to minimize potential secondary side-effects that could be cumulative over large classes of substances (for example, effects on the liver).
I don’t intend to promote any specific substances or interventions here as I don’t give medical advice, nor do I want anything specific to be the focus of this post, but I do want to remind us that just as we can calculate expected values in a utilitarian fashion and get effective altruism as a result, we can do the same for longevity interventions and get a very strong chance at notably increasing our lifespan/healthspan as a result. I do have a list of some of what I take here, but it is definitely not intended to promote anything specific to others.
Why Not?: Potential counter-arguments
Algernon’s Law
Algernon’s Law is sometimes brought up, suggesting that evolution has already put a lot of effort into optimizing our body, and thus we are unlikely to find improvements easily. But, as Gwern notes in the above link, there’s at least three potential ways around this reasoning: interventions may be complex (and/or too far away in the evolutionary plane) and could not have easily been found, they may be minor or only work in some individuals, or they may have a large trade-off involved and cause harm to reproductive fitness.
Although some areas of future longevity treatments may fall under exception one and be complex enough that evolution could not have found them, I would suggest that the majority of today’s potential treatments fall under exception three: evolution optimizes for reproductive fitness, not for longevity, and for this reason there are many interventions which will improve our longevity that it has not given to us already (this is part of why I am more optimistic about longevity interventions than I am about intelligence interventions/nootropics).
For an extreme example of this, it has been noted that castrated males often live longer, and that this is obviously something evolution would not be very interested in exploring. Although this has been found with median lifespan in male mice (maybe in females too?), there is also purported historical data on Korean eunuchs suggesting that they may have lived a full 14-19 years longer (there are definitely potential confounding variables and/or bad data here, but we don’t have RCTs on this in humans for obvious reasons..), and a more recent study in sheep that is also highly relevant: Castration delays epigenetic aging and feminizes DNA methylation at androgen-regulated loci, where epigenetic aging clocks that look at DNA methylation are used in castrated sheep. There are other traits that seem to improve longevity as well, for example decreased height. It seems quite plausible that there are a lot of trade-offs that optimize for strong reproductive fitness early in the lifespan of organisms, which end up costing the organism dearly in terms of longevity. These trade-offs may be involved in many areas such as testosterone, estrogen, growth hormone, IGF-1, caloric restriction, mtor activation, and many others.
Large error in estimating unknown risks
One other counter-argument here is often along the lines of “you are messing with things you don’t understand, and you could be hurting yourself but be unaware of this; the damage may also be difficult to notice, or perhaps only become noticeable at a much later time”
It is true that our understanding of biology is lacking, and therefore also that we are operating in highly uncertain environments. I would be open to evidence that suggests reasoning for why we may be systemically underestimating the unknown risks of longevity interventions, but given how strong the potential upside is, these would have to be some pretty terrible mistakes that are being made. It is often noted how curing cancer may only extend human lifespan by a few years, whereas a longevity improvement of 5% for everyone would provide much more value (and is also much easier to find in my opinion). One could make an argument here that even if I was doing something that notably increased my risk of e.g. cancer, if the expected lifespan increase of this intervention was as much as 1-5%, this could still be a huge net positive for my health! I don’t take approaches that are this extreme regardless, and I try to keep the risk side of my risk/reward ratio low independently of the level of potential reward in attempt to account for this uncertainty. I am also not aware of many interventions that seem to have very high numbers in both the numerator and denominator here, although I am pretty certain that they do exist; I don’t currently take anything that I think has notably detrimental side-effects for the time being.
Is it fair to call this approach Pascallian?
The original nature of Pascal’s wager is that of extreme probabilities resulting in positive expected values, but the numbers that we are operating with are nowhere near as extreme as they could be. It is probably not a good idea to take 10,000 supplements, each of which have a 0.1% chance of extending your lifespan by a year for many reasons (similarly, if 10,000 people that claimed to be God all offered me immortality for a small fee, I would hope to decline all of their offers unless sufficient evidence was provided by one).
As I’m not arguing in favor of taking hundreds or thousands of supplements in the hopes that I strike gold with a few of them, it may be worth noting that ‘Pascallian Longevity’ would be a poor label for my strategy. Regardless, taking just 5-10 longevity interventions with a strong upside potential seems to be significantly more than almost everyone is doing already, so I still stand by my claim that there are many free lunches (free banquets, if you ask me) in this area, and I am very optimistic about the types of longevity interventions we’ll find in the coming decades.
Allulose (sometimes D-psicose) is by-far one of the best ways to add sweetness to home-cooked meals in a healthy and low-calorie way. As an epimer of fructose, it has been steadily gaining popularity within the last few years, and not without good reason! Allulose is not only nearly calorie-free, but also decreases blood glucose levels with meals, and seems to have a wide range of potentially beneficial effects.This post is a short summary of why allulose is so appealing over sugar and other sugar substitutes.
70% as sweet; 100% as white and crystalline
Overview of Allulose
Allulose is found naturally in wheat, figs, raisins, maple syrup, and molasses, although in relatively trace amounts. It has around 10% the calories of traditional sucrose and can be manufactured from fructose. It’s around 70% as sweet as sucrose (regular sugar), but has a similar taste and feel, which is a large factor behind why it makes a great substitute (or partial substitute) for baking or dissolving into things. The taste of Allulose has a more natural and relaxing quality than some other sugar-replacement options such as xylitol and erythritol, which are both sugar alcohols, but generally have a ‘cooling effect’ (often likened to the aftertaste of consuming mint, which allulose conveniently lacks).
Allulose is also an actual sugar (not a sugar alcohol or other compound), and has similar browning properties to sucrose via the Maillard reaction. One downside to mention is that it does seem challenging to keep some styles of baked goods crunchy with allulose as the only sugar; while it definitely seems to be one of the best options for sweetening drinks, yogurts, ice creams, cakes, and so on, it may not be the best option for super-crunchy cookies (although can make great softer ones!). This seems to be due to allulose not crystallizing when it cools, its ability to hold more moisture, and that it is more soluble in liquids than sucrose; hence it being a great fit for drinks, sauces, and spongy baked goods.
Allulose was designated asGRAS by the FDA in 2019, so is still relatively new to the market compared to many other sugar substitutes, although has been gaining significant popularity for the short period that it has been available for general usage in foods. I’m sometimes now able to find allulose for sale in a supermarket or included in a sweet good (and it is also now being used in products such as Soylent), although its usage is still a small fraction to that of sugar and corn syrups. It can easily be purchased on Amazon for around $10 per lb (regular sugar is generally closer to $1-2 per lb, so it is quite a bit more expensive if you happen to use very large amounts of sugar).
What Sets Allulose Apart
Why might we want alternative sources of sweetness from sucrose to begin with? Although much has been said about the ways sugars are (in some cases) potentially harmful, it seems reasonable to posit that there are two qualities of a diet with high sugar content (remember, this means any typical western diet!) that are undesirable: firstly, the high caloric content of sugar, which makes over-eating significantly easier and therefore contributes to obesity, and secondly, the effects of sucrose on blood glucose levels and thus insulin resistance, which contributes to diabetes and metabolic syndrome.
As we would hope from an alternative to sucrose, allulose doesn’t cause an increase in blood sugar. The reason for this is that it is not absorbed and digested by the gastrointestinal tract, but rather processed by intestinal bacteria. For the most part this is a good thing, and is what enables allulose to both be low-calorie and to not be converted to glucose in the blood stream. The downside of this is that for some people, especially if consumed in large enough quantities, it can cause mildly discomforting side effects such as flatulence, subpar digestion, and abdominal discomfort. This is much more likely to occur if you, for example, eat an entire batch of allulose cookies by yourself (who would do such a thing..!?), rather than simply use it to sweeten a drink or a snack. While I haven’t experienced anything negative myself, everyone is certainly very different when it comes to food.
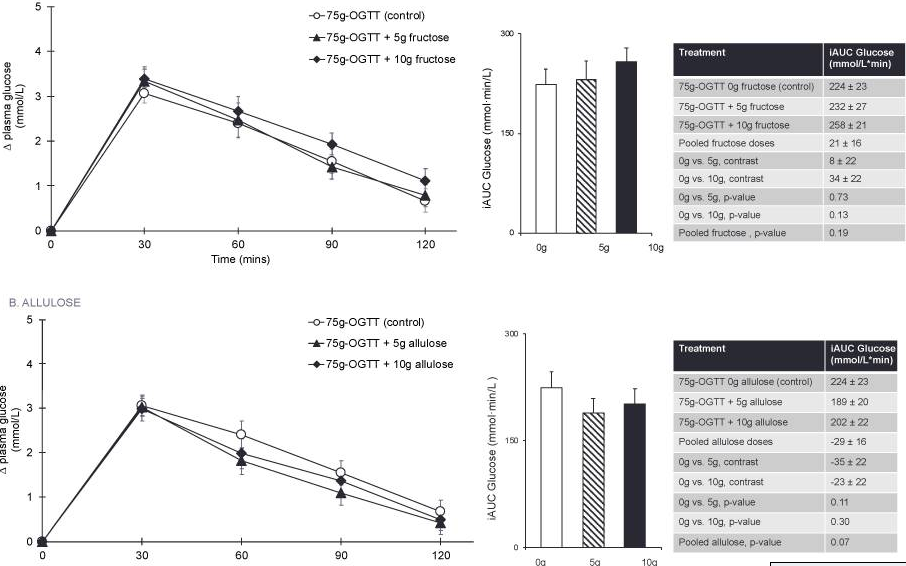
But, it gets much better than this! Allulose not only doesn’t increase your blood sugar, but actually decreases it! It does this by inhibitingalpha-glucosidase (along with several other similar enzymes), which is an enzyme that breaks down starches and disaccharides into glucose (i.e. causes carbohydrates to lead to blood glucose spikes). Other well-known inhibitors of alpha-glucosidase include acarbose, a popular and simple diabetic drug which significantly extends lifespan in mice and has the exact same potential side effect profile as large allulose doses (and in my opinion is probably very good for most people to be taking, perhaps extending human lifespan via the same mechanism of action as in mice), and sweet potatoes (source, another source). Thus, adding allulose to meals that contain carbohydrates will result in less of a blood glucose spike than if allulose had been excluded.
Comparison of blood glucose area under curve for small quantities of fructose vs allulose (source: figure 1)
There’s now quite a few studies showing this in humans (and dogs and mice!), with allulose consistently attenuating the postprandial glucose levels both in diabetic and regular adults (effect sizes are often larger in pre-diabetic and diabetic individuals, as is often the case here).
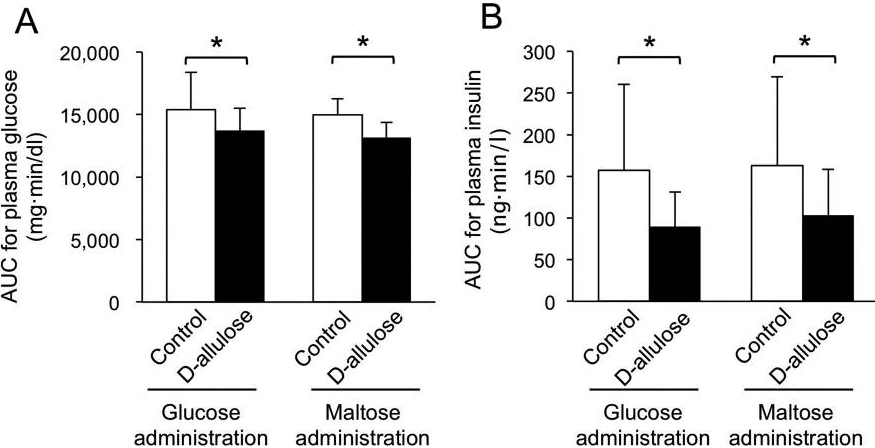
Allulose blood glucose and insulin areas under the curve in comparisons with other sugars (source: figure 2)
But wait, there’s more!
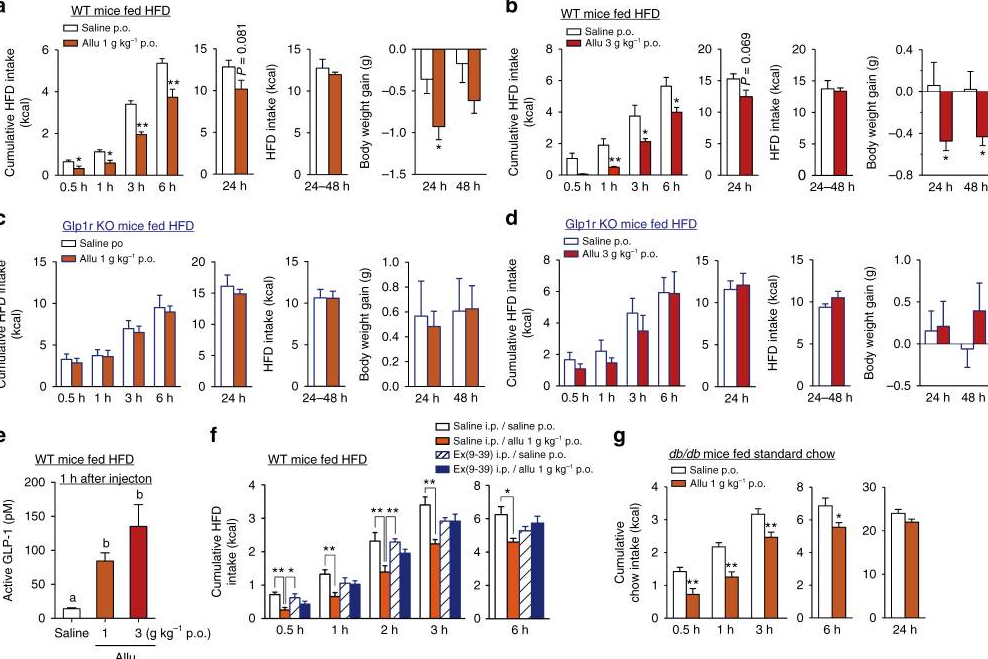
Several studiesalso appearto showlower plasma triglyceride levels and improved lipid profiles (perhaps via the lowering of hepatic lipogenic enzyme activity, maybe involvingSCARB1, but probably many others as well), decreased feeding (perhaps via agonizing glucagon-like peptide-1), enhanced fat oxidation, and a reduction in inflammation related to adipokine and cytokine plasma levels (one paper claims this is partially due to down-regulating gm12250 in mice, but if this applies to humans it may be a side-effect of more upstream metabolic changes more so than specific agonism/antagonism, although as is the case with most foods, things get absurdly complicated very quickly with the amount of pathways involved).
Allulose resulting in reduced feeding in high-fat diet obese and diabetic mice (source: figure 3)
It’s worth noting that several of the above studies (particularly ones that attempt to hone in on specific mechanisms of action) are in mice, and in fact, we could go much further if we want to look at mice; it’s trivial to find many more potentially favorable results such as “Not only metformin, but also D-allulose, alleviates metabolic disturbance and cognitive decline in prediabetic rats” or “D-allulose provides cardioprotective effect by attenuating cardiac mitochondrial dysfunction in obesity-induced insulin-resistant rats“. Although there is less (and sometimes conflicting) evidence for e.g. improved lipid profiles in humans, there is certainly more than sufficient evidence of allulose’s effect on reducing blood glucose levels and overall calories consumed, from which we would naturally expect many other beneficial effects to follow. Searching for allulose on pubmed results in a wonderful selection of studies showing very consistent outcomes in this area, and it thus seems plausible that, at the very least, we would see significant reductions in diabetes and obesity if allulose were to be more widely adopted in consumer food products.
Conclusion
In general it seems like replacing sugar with allulose will result in fewer calories consumed, a lower risk of obesity, lower blood glucose (average and area under the curve, sometimes peak) levels and thus improved insulin resistance and a lower risk of diabetes and metabolic syndrome, and potentially some other beneficial effects (which may or may not apply in humans, but if allulose improves your diet and lowers your food intake, I would not be surprised to see improved lipid profiles and a reduction in inflammation, even if entirely for indirect reasons, e.g. cooking at home with allulose instead of purchasing processed foods from the store. It’s also worth noting that while some of these benefits are a direct result of allulose consumption, many are also partially from a reduced intake of sugar and calories – similar to how cutting down on your sugar intake would offer many benefits).
It’s quite possible that if a notable fraction of other sugars in our diet were to be replaced with allulose, the amount we would gain both in QALYs and dollars saved via the resulting reduced healthcare burden would be extremely favorable. Allulose is still relatively new to the market, and as it is also much more expensive than sugar or corn syrups, its future market penetration may be relatively limited by consumer preferences. Regardless of its presence in our broader food ecosystem, you can start experimenting with it yourself today! (Amazon search results page link, in case this saves you 10 seconds)
I usually use allulose to sweeten drinks, greek yogurt, and sometimes add it to sauces or baked goods in small quantities. I’m also pretty interested in glycine and think it may be something that most of us should be having a lot more of as well (some notes on this in the glycine section on my supplements page), but consider it outside the scope of this article for now. Lastly, if the idea of significantly reducing the glycemic index of your meals is appealing, I strongly suggest looking into acarbose – it is a much stronger inhibitor of alpha-glucosidase, well-tolerated, and also relatively cheap.
If you enjoyed this article you might also enjoy my supplements page which discusses many other ingredients and drugs that I find interesting with respect to longevity. Feel free to reach out with any comments or corrections via any communication method on my about page, thanks for reading!
This document is an updated list of most of the supplements/drugs that I take daily, as well as notes on some other interesting substances. It contains information on exactly what I take, how much of it, how much it costs, and some information on the substance which should roughly explain my reasons for taking it.
May 7th 2024 update: I have replaced many of the pills in this post (but not all of them!), with pills from Blueprint, although I don’t consume any of the auxiliary products. I would strongly suggest reading my post and review of Blueprint as it is now an essential addendum to this post. It saves quite a bit of management time as well.
The first list contains supplements I take daily, with the second list containing supplements that I do not take daily but that nonetheless seem interesting, while the third list contains supplements that are interesting, but that seem less suitable for safe human consumption or speculation. As of 2023, many supplements on my list have been discontinued, and this is mentioned next to the dosage.
The focus of my supplementation is to find substances that are both very safe and also have a notable probability of improving health, lifespan, well-being, or productivity, with the ultimate goal being to significantly slow aging, even if it’s difficult to do at this time. I don’t take many nootropics as I don’t think there’s much room for intelligence improvements just from ingesting simple compounds (evolution has already put quite a bit of time into making us smart), with the exception of treating some deficiency or other issue, or improving productivity/concentration, which definitely possible (see: caffeine, modafinil, adderall, many others), but distinct from intelligence. It is worth noting this list is very specific to myself: if I had a perfectly optimal diet and lifestyle, I would likely take next to zero supplements. Like most mortals, my diet and lifestyle are definitely not perfect (and indeed, even knowing what a perfect diet would be for yourself can be intractable on its own), thus there’s always room for improvement.
This post is not an attempt to convince anyone of something
specific or to suggest anything specific, but I have decided to
publish it publicly in order to better keep myself accountable for my
reasoning, receive potential feedback, and to otherwise share some
potentially useful short summaries of information. Concordantly, I’m
not a doctor and this post contains no medical advice or suggestions.
Which supplements, if any, one should take, is a very personal
matter, as it is dependent upon many unique traits such as one’s
age, diet, lifestyle, genes, risk preference, finances, and more.
Notes on supplements
Section tl;dr: most supplement marketing tactics, websites, videos, brands, etc, are bullshit. Do your own research, ask questions, and be quantitative.
Although there are a lot of supplements that would be beneficial to many people, caution must be exercised both with research and purchasing. Supplements in the United States have very little regulation, with some sellers having poor quality control, fraudulent research, marketing, claims, and poor ingredient composition and sourcing. The supplement industry is worth billions of dollars and has many bad actors incentivized by profit over truth, so time and care must be exercised in order to find out what works best for you personally. Certainly, research can be found promising positive effects from thousands of various substances – but taking all of them would be impractical, expensive, and likely downright harmful.
It’s also important to pay attention to brands as well as to think logically about which supplements have quality differentials that are worth paying more for. For example, Vitamin D and Glycine are easy to synthesize, and it’s likely that cheaper versions of these supplements are just as good as more expensive versions. This may not be the case for a supplement like fish oil however, which is derived from complex living organisms that vary significantly on factors such as their environment, diet, quality controls, the types of fish used, and so on.
Concordantly, one of the strongest criteria I look for in most supplements is safety, which many times (not always!) comes alongside popularity and/or significant research affirming the safety of compounds. As many supplements offer marginal benefits at best, it would be irrational to purchase and consume them if they had a good chance of causing harm, as this would easily cause them to fail a basic cost/benefit or risk/reward analysis (there’s definitely some cool compounds that have very high coefficients in both the numerator and denominator of their risk/reward ratio too, so careful decision making is required).
Ideally one should attempt to find quantitative measures to
objectively evaluate if a substance is really helping them in the
desired manner. In some cases this is both easy and cheap to do, for
example with Vitamin D supplementation, which costs only a few cents
a day, does not need to be compared to a placebo, and can be tested
for in your blood for as little as $30. In other cases, proper
testing is difficult or impossible and may require significant effort
and time for very little benefit. Keeping one’s lifestyle, diet,
and other factors a perfect experimental constant is certainly
difficult, as is performing blind experiments on yourself, collecting
and analyzing data, and finding the proper quantitative desideratum
to test yourself on to begin with; testing if something specific has
definitively made you slightly smarter, happier, healthier, more
productive, or extended your lifespan, is certainly difficult if not
occasionally impossible to do in a scientifically rigorous manner
with a sample size of one.
Lastly, which supplements benefit an individual is a very personal matter. Vegans may want to take some supplements that are found in meat. Carnivores may want to take some supplements that are found in plants. Supplements that may benefit the elderly or those with common conditions such as hypercholesterolemia or diabetes often seem to be much less useful for otherwise healthy individuals. Indeed, for individuals that have many health conditions including the elderly, there’s significantly more that can be gained from supplementation, as there are many more problems that can be improved upon (although there are also be more risks as well). Supplements will effect someone differently depending on their weight, age, genetics, health, diet, and many other factors.
This means that it’s a bad idea to copy any individual’s routines completely, even if it’s a lot of work to do your own planning, research, and testing. It is also worth mentioning that the word ‘supplement’ is used here as a relatively generic word, simply meaning that the substance is only regulated as a food within the United States and thus requires no prescription (unless otherwise mentioned), but also offers few guarantees in terms of efficacy or consistency.
If you take 2 or more pills a day, the best pill organizer+dispenser by far is this (Image from Amazon reviews)
See also
If you find this page interesting, here are some similar pages from others that you may enjoy:
Information: Vitamin D3 [Examine, webmd, Wikipedia] (colecalciferol) is a vitamin made by the skin when exposed to sunlight. It’s a common deficiency and is very cheap to fix. The benefits of supplementation are generally found to be minor (it’s still a bit controversial if supplementation is beneficial at all, although I lean towards yes personally), but as I was notably deficient and it’s one of the cheapest supplements, it’s an easy choice for me. There is a lot of literature on Vitamin D, and many highly-powered studies including meta-analysis will often find only minor beneficial effects, but there are also quite a few studies that show notable benefits, including many related to covid as of late 2020. As noted above, this is also an easy supplement to receive a blood test for and ensure you’re taking the optimal dosage. I take half of my vitamin D earlier in the day without a meal, and the other half with my food, contrary to most other supplements. See also: Gwern on Vitamin D as well as on it harming sleep if taken at night
Name: Vitamin B6
Dosage: 1.4mg (included in BP)
Cost/Day: $0.04
Information: Vitamin B6 [Examine, webmd, Wikipedia]. This is included in other supplements I have and is otherwise not notable.
Name: Vitamin B12
Dosage: 125mcg (included in BP)
Cost/Day: $0.04
Information: Vitamin B12 [Examine, webmd, Wikipedia] (vitamin B3). This is included in other supplements I have and is otherwise not notable (although if you’re on metformin or a few others I used to try it’s better to add it, else unlikely to be deficient).
Name: Vitamin C
Dosage: 500mg
Cost/Day: $0.03
Information: Vitamin C [Examine, webmd, Wikipedia] (ascorbic acid) has a variety of effects, and being a vitamin, is an essential part of a human diet. I supplement vitamin C in order to fix a tested deficiency. I’m rarely deficient but it doesn’t hurt.
Name: Fish Oil
Dosage: 1-3g+ (depends on diet and estimated omega-6 intake)
Cost/day: $0.10 (1g)
Information: Fish oil [Examine, webmd, Wikipedia] (omega-3 EPA+DHA) is another common and cheap supplement. Although many studies find minor or sometimes no benefits, many others find a large amount of diverse improvements, even if they are minor. It’s likelythat the ratio of omega-6/omega-3 you consume is important, with most people consuming far too much omega-6 (which won’t hurt to reduce regardless) and not enough omega-3, so dosing of fish oil should be based on your diet, which is easily more than an order of magnitude more important to begin with.
Similarly, it’s probably good advice to 1) reduce fried food intake, 2) replace oils high in linoleic acid such as safflower and sunflower oils with oils that have much less such as coconut oil and olive oil (2021 edit: I am less sure about this than I was before, although I still lean towards it myself Deciding which oils/fats (and with what / prepared in which manner) are bad for you continues to be an extremely hard problem. See A Comprehensive Rebuttal to Seed Oil Sophistry for an example of a comprehensive potential counter-argument in the great seed oil/fat debate) and 3) increase my supplementation of high-quality omega 3s (fish oil) when I think I’ve had more omega 6s. For example, if I do decide to eat a lot of fried food, I take several fish oils, compared to only 1-2g normally. I also like to note that fish oil seems to be one of the supplements worth spending a bit more money on – quality is high-variance and of higher importance, and unlike other supplements which can trivially be synthesized, the production processes of fish oil vary greatly depending on the company and product. Also see this review on pubmed and this summary on Wikipedia
Name: Garlic
Dosage: 1-3g (included in BP now)
Cost/day: $0.02 (1g)
Information: Garlic [Examine, webmd, Wikipedia] is another popular and cheap supplement. There’s good evidence that it improveslipidprofiles, may help with some cancerrisks, and may have other very minor benefits (may activate AMPK too?). The most desirable compound in garlic is allicin, which is diluted in garlic that is microwaved, boiled, or aged. Dosage should be based on which type of garlic is being consumed. As many people enjoy the taste of garlic, it’s a good candidate to include in meals as well (which is probably optimal for most things, resulting in notably higher bioavailability on average).
Name: Olive Leaf
Extract
Dosage: 500mg (discontinued, decided it was too low-value)
Cost/day: $0.02
Information: Olive Leaf Extract [Examine, Wikipedia] is a cheap and easy way to hopefully mimic the benefits of olive oil, as the leaves of the olive tree contain good amounts of relevant olive phenols such asoleuropein. It may still be better to consume olive oil instead, which is still a great thing to add to meals, but with such a low cost, this seems worth inclusion to me. I am not particularly excited about this supplement but have included it regardless.
Name: Magnesium Citrate (replaced with magnesium glycinate)
Dosage: 250mg (magnesium glycinate: 1500mg)
Source: $0.05
Information: Magnesium [Examine, webmd, Wikipedia, Gwern] deficiencies are moderately common (up to 45-60%) and easily fixed. Fixing a magnesium deficiency is cheap and seems to offer quite a few minor general benefits, and also sleep and anxiety improvements for some. Depending on your diet, supplementation may be unnecessary. Magnesium comes in a lot of different forms so close attention is needed when purchasing. I stick to citrate as it makes dosing easier, has good bio-availability, and is unlikely to cause digestion issues. The above Gwern link is a great resource on Magnesium as well. This is also another supplement that is easy to get before and after blood tests for to see if your intervention performed as desired.
If you want to have both magnesium and glycine, magnesium glycinate can be purchased which contains both, generally in a ratio of ~14% magnesium to ~86% glycine. This can be a great supplement to take before bed.
Name: Vitamin K2
MK-7
Dosage: 100mcg (sometimes included in BP)
Cost/day: $0.00
Information: Vitamin K [Examine, webmd, Wikipedia], like most vitamins, is primarily beneficial for those deficient in it, so it is best to examine your diet thoroughly and/or be tested. There are several forms of vitamin K, and also several forms of vitamin K2. Vitamin K2 MK-7 seemstobe one of the best forms to take in general, although K1 has decent evidence in favor of it as well, depending on one’s circumstances.
Name: Glucosamine
Sulfate
Dosage: 1-3g (often paired with MSM, back on as of Oct 2024)
Cost/day: $0.19
Information: Glucosamine [Examine, webmd, Wikipedia] is an amino sugar derived from shellfish that is commonly taken by the elderly to improve joint functionality and reduce pain. Glucosamine extends the lifespan of some mammals in studies, potentially in ways that are evolutionarily conserved, activating AMPK and therefore having slight similarity with metformin. Glucosamine may also induce autophagy via an mTOR-independent pathway, which may be the mechanism of action for its effects on lifespan. Due to its popularity as a supplement we can be relatively sure of its safety as well. Chondroiton is commonly included with glucosamine supplements, which appears very uninteresting for my own purposes, so I look for pure d-glucosamine/glucosamine sulfate, which is generally cheap.
Name: Lithium Orotate
Dosage: 5mg (included in BP)
Cost/day: $0.08
Information: Lithium [webmd, Wikipedia] is a metallic element that is often found in foods such as legumes, grains, vegetables, and in some places, drinking water. Lithium is generally present in most diets in notable quantities, and in slightly larger quantities in diets such as the Mediterranean diet. For purposes such as mine, it is supplemented at low doses, which is much different (~1/100th the dose) from the doses sometimes prescribed for some psychiatric disorders. Lithium reduces mortality, stabilizes mood, and promotes longevity, likely via multiple pathways, although the specific mechanisms of action are difficult to discern and more research is needed. As I was tested for lithium and had a very low concentration in my blood, I decided it was worth it to supplement it n low doses.
Name: Glycine
Dosage: ~5-10g+
Cost/day: $0.20
Information: Glycine [Examine, webmd, Wikipedia] is an amino acid that is often supplemented to improve sleep. Better sleep is formidable by itself, but some studies find that it increases lifespanin organismsvia methods that may be evolutionarily conserved. Although glycine is present in some foods and is also synthesized by your body, it may bethe case that glycine deficiencies are technically common in humans, as the amount that is able to readily be synthesized in-vivo is sub-optimal. This may be relatively asymptomatic from an individual perspective and only manifest itself via a slight probabilistic decrease in healthspan/lifespan, although users often notice quite a few improvements besides just better sleep. Given its heavy involvement in collagen, I wouldn’t be surprised to see skin benefits over the long-term. Glycine may improve insulin sensitivity and other similar metrics. There may be somelongevitybenefits of a diet low in methionine (meat, fish, eggs, etc) as well, which may be related to one’s effective glycine/methionine ratio. I still consume a lot of methionine from common sources such as chicken breast, so this is another potential way in which glycine could be beneficial. Glycine appears to be very safe, even in larger doses, and is relatively cheap, more so as a powder, as is the case of most substances. See also Induction of glutathione biosynthesis by glycine-based treatment mitigates atherosclerosis
I often take glycine in powder form, which makes it easy to consume arbitrary doses (including the ability to add it to drinks or meals if desired), and notably cheaper than buying large amounts of pills, which are generally 1g each at most (you can’t fit more in a pill). On days where I consume a lot of meat such as beef, I take significantly more glycine. This is partially an attempt to optimize my diet’s methionine/glycine ratio, but also intended to do a better job at mimicking what a more traditional consumption of animal meat might have been like, from an evolutionary perspective, which would have included much more glycine than most of us receive in the common cuts of meat that consumers generally use. As a side note, glycine does taste sweet and dissolves in water, so it’s a great addition to tea or coffee.
(Dec 2024 update) I also supplement collagen peptides. Collagen peptides are a more popular supplement which contain 1/3rd glycine along with other amino acids such as proline and hydroxyproline. Glycine seems to generally be the bottleneck for sufficient collagen synthesis, however it seems like collagen peptides in some cases don’t fully break down into the constituent amino acids and may thus offer other signaling benefits, e.g. “telling your body to produce more collagen”. As they’re obviously low risk and likely very good for you, I currently supplement both collagen peptides and glycine on a daily basis.
Regardless, given glycine’s near-flawlessly safe and simple profile, there should be zero harm in having a bit too much. My larger dosage was arrived at from a combination of the papers linked above (and linked to by those links), as well as some reasoning about my diet (high in methionine) and lifestyle. Unfortunately even with a blood plasma test of amino acid concentrations, it’s difficult to know if this is the optimal dose for human longevity, or if it is even helpful at all to begin with, but the cost/benefit analysis here still seems to lean heavily into the green. As a simple and common amino acid, it seems pretty difficult to hurt yourself with glycine, so even taking 10-50g a day shouldn’t be harmful.
Creatine
Name: Creatine
Dosage: 3-5g
Cost/day: $0.10-0.18
Information: Creatine [Examine, webmd, Wikipedia] is an organic compound used in the recycling of ATP in humans. It can be found in notable amounts of muscle meat and can also be synthesized in humans via glycine, arginine, and methionine. Creatine is a very popular supplement for athletes with strong evidence that it notably increases power output and lean mass, with some evidence that it can offer minor improvements in related areas such as recovery, fatigue, and some biomarkers that are positively associated with quality anaerobic exercise. It’s very safe, has little potential for any side effects, and is relatively cheap.
Name: Allulose
Dosage: 0-10g+ (varies, uncommonly used as a sweetener with some meals)
Cost/day: $0-0.50
Information: Allulose is an amazing alternative to sugar with 90% fewer calories and the ability to decrease your blood sugar in response to high-carbohydrate meals. I wrote a full post on Allulose here
Name: Bacopa
Dosage: 445mg (discontinued, likely low value)
Cost/day: $0.09
Information: Bacopa [Examine, webmd, Wikipedia] is an herb that seems to offer reliable but likely very minor improvements to some areas of memory and generalcognition. Effects are likely difficult to notice without rigorous placebo-controlled self-testing, but it is relatively safe and cheap regardless. Digestive side-effects aren’t uncommon, as is the case with many herbal supplements. In the future I’d like to replace my bacopa with a placebo and attempt to look for differences in quantitative cognitive performance metrics such as my anki recollection, but performing this experiment well is difficult, both because the effect is very minor and because a proper experiment with n=1 is very difficult. I don’t think bacopa is likely to be a big deal, but I’ve added it for now. As of 2021 I sometimes don’t take this, as it may result in slightly poorer digestion, and the benefit was marginal at best, but I have left it on this list for now.
Name: Ashwagandha
Dosage: 470mg (occasionally discontinued due to potential digestive side-effects)
Cost/day: $0.15
Information: Ashwagandha [Examine, webmd, Wikipedia] is an herb that offers potential anxiety and lipid profile improvements. Some users report that it reduces anxiety and stress significantly, with some studies showing up to a 28% reductions in cortisol (in subjects with elevated levels). Lipid improvements can also be notable, with some studies showing a 10% reduction of total cholesterol, even in healthy subjects. As an uncommon herbal supplement, digestive side effects are a notable probability. Ashwagandha is likely worth trying if you feel that you have untreated anxiety, you never know when you’ll get lucky with how much of a benefit you receive from some things. Although not scientifically rigorous, it did appear like the periods during which I took ashwaganda resulted in a notably improved lipid profile, consistent with what many studies have shown. I’d like to test this on myself in an n=1 RCT both for lipids and for potential relaxation/anxiolytic effects, but haven’t gotten around to it.
Name: Fisetin
Dosage: 0-1500mg (varies, intermittently/rarely taken, but now included in BP at 100mg/day)
Cost/day: $0-3.80 (varies)
Information: Fisetin [Wikipedia] is a plant flavonol that is found in several vegetables and fruits, with the highest concentration being found in strawberries. Fisetin is a sirtuin-activating compound and has extended the lifespan of yeast, worms, flies, and mice. It has been shown to be a strong senolytic agent and may induce apoptosis and other effects via the PI3K/AKT/mTOR pathway. I do not take it every day and am quite uncertain about what the right regime for supplementation should be for it, but currently take ~1,500mg of it for 4 days continually once every few months. This likely has room for improvement and may change in the future. I’d like to write more about fisetin in order to justify this, but haven’t yet found the time. Here’s a single picture of a pretty mouse instead.
Astaxanthin has increased
the life span of C. elegans by 16-30%, with the authors stating
“These results suggest that AX protects the cell organelle
mitochondria and nucleus of the nematode, resulting in a lifespan
extension via an Ins/IGF-1 signaling pathway during normal aging, at
least in part”. While this is certainly interesting, expecting such
a lifespan increase in humans is far too optimistic from this case
alone.
However, Astaxanthin may
be able to activateFOXO3
in humans, an important
gene for human longevity which is present in many centenarians.
Some other well-known natural compounds such as resveratrol
and curcumin
also interface with FoxOs, although these substances are still
relatively speculative as far as anti-aging effects in humans go,
even if they do have many strong supporters.
There’s some other interesting potential effects of astaxanthin,
with some papers showing that it increases
neural stem cell proliferation and may be useful to help curb
dementia, and other papers showing that it can improve
skin health and appearance, leading it to become an ingredient in
some cosmetics.
Astaxanthin appears to be very safe in humans and is a relatively popular dietary supplement, with a market estimated at over $500M USD annually, although the majority of this supply is used as a component in animal feed and cosmetics.
Name: Curcumin
Dosage: 0-500mg (often discontinued, included in BP)
Cost/day: 0-$0.17 (varies)
Curcumin [Examine,
webmd,
Wikipedia] is a
pigment found in tumeric.
Curcumin’s strongest benefit seems to be the reduction
in inflammation that it offers, although there appear to be some
other areas that may be improved as well such as lipid profiles,
mental health, potentially improved digestion, and reduced pain with
some conditions such as osteoarthritis.
It may exhibit a notable anti-tumor
effect via apoptosis. It seems relatively safe, although has low
bio-availability, so is often taken with substances to increases its
availability such as piperine, or taken in an otherwise proprietary
formulation that generally has some type of oil that improves
bio-availability instead. As inflammation is important in aging and
many other diseases, it’s something that is nice to be aware of.
I only sometimes take curcumin depending on my inflammation levels, generally measured via c-reactive protein.. When it is negligibly low, I stop taking it, and if I ever see it creep up in blood test results, I resume supplementation. Curcumin can be potentially tough on the liver, and in large doses has a greater potential to cause adverse affects. Some papersshowquiteafew potential drug interactions that can occur by taking curcumin, especially in larger doses, and via a variety of mechanisms, including its affect on platelets and potential interactions with enzymes such as CYP3A4, potentially affecting the metabolism of a large amount of drugs.
Name: Berberine
Dosage: 1.2g (discontinued, replaced with metformin which was then deprecated)
Cost/day: $0.28
Information: Berberine (Examine, webmd, Wikipedia] is an extract from various plants. It appears to be a pretty strong natural mimetic of metformin, a popular drug for diabetes with many alluring potential anti-aging properties. It often improves lipid profiles and blood glucose, and thus may have many of the long-term benefits that metformin may have. Concordantly, the possibility for digestive side-effects is relatively high, and it’s sometimes taken several times a day in smaller doses as a result. Examine suggestions that it also inhibits enzymes such as CYP2D6 to some extent, which could lead to undesirable interactions with some drugs. It’s likely better to be on metformin than berberine, as drugs are kept to a significantly higher regulatory standard than supplements are and we have much more data on users of metformin.
Name: Caffeine
Dosage: 50-200mg
Cost/day: $0.10
(much higher If drinks are considered)
Information: Caffeine [Examine, webmd, Wikipedia] is something you likely don’t need an introduction to. I try to keep my dosage relatively low to avoid issues with tolerance, using a combination of coffee, tea, or caffeine pills, depending on the amount desired and my mood. When taking 100mg or more of caffeine, I generally have 100mg of L-theanine as well.
Dosage: 0-200mg, (not taken often, 100mg if taken generally)
Cost/day: $0.20
Information: L-theanine [Examine, webmd, Wikipedia] is an amino acid that is present in tea leaves which is often combined with caffeine for supposedly synergistic effectsoncognitionandmood, improving the upsides of caffeine while helping to ameliorate some of the potential downsides. I generally only take it if I’m having more caffeine than average on a given day, since I keep my caffeine intake pretty low.
Name: Melatonin
Dosage: ~300mcg or less (not taken consistently)
Cost/day: $0.04
Information: Melatonin
[Examine,
webmd,
Wikipedia,
Gwern] is a hormone
secreted by the pineal gland with an important role in regulating
your sleep cycle. Melatonin production can be suppressed in many
individuals that are otherwise healthy, for example by exposure
to blue light from computer screens before bed (which solutions
like the program f.lux and blue-light blocking glasses attempt to
solve). The generally accepted benefits of melatonin are a reduction
in the time to fall asleep, although some individuals claim that it
reduces their need for sleep as well (often by 15-60 minutes). For
those with sleep conditions such
as insomnia or jet
lag (or just being older in many cases), melatonin can be a much
greater aid in improving sleep and quality of life.
One meta-analysis
(K=10, N=653), found melatonin supplementation may have helped
significantly reduce some instances of cancer mortality (R = 0.66
after 1yr). Some
studies also find improvements
in gastroprotection, healing
and reducing the rate of stomach ulcers.
Melatonin has
increased the
lifespan of some mice by 18%, primarily given as a supplement
later in life in an attempt to give older mice more effective pineal
gland functionality (directly giving older mice the pineal glands of
younger mice was also performed, which also was very beneficial).
Melatonin levels similarly decline
with age in humans (as most important things do), and
supplementation may be increasingly
beneficial as one ages.
The proper dose of
melatonin to take varies between individuals and many melatonin pills
for sale are dosed too high (5-10mg), so approximate
self-experimentation can be used such as starting with 0.5mg and
increasing your dosage until benefits are noticed. The above link to
Gwern’s website on Melatonin points to a good in-depth analysis
that is worth reading as well.
A few other things you may want to be aware of if you’re interested in melatonin is that you can buy delayed-release and extended-release versions easily otc. Additionally, you can use a beta-blocker like propranolol to inhibit melatonin synthesis to assist in circadian rhythm regulation.
Name: Spermidine
Dosage: ~1-10+mg (various sources, now included in BP, previous source was wheat germ)
Dosing for spermidine is difficult. It’s obviously very safe, but 1mg is likely not enough for the level of effect that we want. The average daily nutritional intake of spermidine varies from 7 to 25mg, and we can see how much one might want to consume for blood levels of spermidine to increase by 39%: perhaps 10mg per day (calculated by multiplying the 66g of natto consumed per day by its approximate spermidine content of 150mg/kg to yield 10mg per day). Although we don’t have plasma concentrations of spermine and spermidine in humans in relation to mortality, this is available in several mice studies. I need to spend more time on this, but I think one might want to supplement as much as 5-20mg of spermadine per day, assuming that it’s not present in their diet in notable quantities already (which is quite possible, as some Mediterranean, Japanese, and other diets contain notable quantities of it).
I currently consume spermidine via wheat germ, which seems to have around 243mg/kg of spermidine in it. If I wanted 10mg a day, this would result in having to consume 41g of wheat germ per day, which although feasible, is a bit tedious, potentially unsavory depending on the method of consumption, and would also result in an additional 164 calories consumed per day. There are some spermidine supplements on amazon, but I am not sure that I trust any of them very much (with the most recent one having the most obvious fake reviews I have ever seen on a supplement), and many of them are simply wheat germ inside of a capsule, which is not only likely to be an insufficient dosage, but also much more expensive. It may be worth mentioning for some readers that spermidine is also present in human sperm, but not in enough quantities to warrant consumption unless you consume copious amounts of it (~0.1mg per ejaculation, assuming 3.5mL and 31ug/Ml).
Information: Metformin [webmd, Wikipedia] is a prescription drug for diabetes and is one of the most popular drugs taken by those interested in longevity, often taken for this purpose by individuals without diabetes. Metformin is said to mimic some of the potential benefits of caloric restriction. It increases the lifespan of mice, increasing AMPK activity and antioxidant protection, resulting in reductions in both oxidative damage accumulation and chronic inflammation. Lifespans of other organisms such as silkworms and nematodes are also increased. There exists a vast literature on Metformin with respect to its mechanisms of improving longevity apart from just this; it’s currently the most popular drug taken to combat aging.
Due to the prevalence of diabetes, Metformin has over 80 million users (the vast majority taking it for diabetes), which gives us wonderful data on its safety, with its side effects rarely including anything besides minor gastrointestinal issues. Metformin is also cheap, costing only $5-$25 a month in the United States. For the above reasons and many others, Metformin appears to be one of the best candidates for an anti-aging drug, leading it to become one of the only drugs making clinical progress in this area with trials such as TAME (Targeting Aging with Metformin). Metformin deserves a larger write-up than I’ve given it here, so you’re encouraged to perform your own research on it (just as you should for anything written about on this page).
For long-term Metformin usage, be sure that you are not hypoglycemic, as well as that your levels of vitamin B6 and B12 are in acceptable ranges, as deficiencies in these are slightly associated with Metformin usage. Metformin may also diminish some health improvements from exercise, and although more research is needed, this factor should be considered for non-diabetics considering Metformin usage. See also: Gwern on metformin
Name: Acarbose
Dosage: varies greatly, infrequently taken at the start of meals with high carbohydrates
Cost/day: $0-$1
Information: Acarbose is a simple diabetic drug which inhibits alpha glucosidase, causing your glucose to spike less than it normally would when ingesting carbohydrates. It is very safe and common, especially in countries such as the United States. Various studies onacarbose in mice have consistently shown it to expend lifespan, sometimes as high as 22% in males, generally much less in females. The probability this applies to humans is, in my opinion, moderately likely, although it is unlikely to be nearly as strong of an effect. Although mice have a lot of similarity with humans (more than many would expect!), their digestive system and diet are more dissimilar than most other categories. With that said, this drug is very safe and provably reduces the glucose spikes in your blood that occur when ingesting large amounts of carbohydrates, which in general seems to be a good thing. It therefore has a lot more potential when taken at the start of eating a large pizza rather than a normal meal (unless pizza is your normal meal, in which case it’s hard to blame you, but you should probably eat other things as well).
Name: 17-α-estradiol / estradiol valerate
Dosage: 0 mg / varies
Cost/day: $0-1
Description: 17-α-estradiol (a non-feminizing form of estrogen) significantly extends male mice lifespan, and this may apply to humans as well. This section turned long so I turned it into its own post. I currently micro-dose estrogen and am experimenting with some other potential solutions here myself; I’d like to write more on this and on related HPG interactions and estrogens/androgens in general. Past links included under this.
I’ve messed around with quite a few hormonal profiles but would like a lot more research in this area, especially on SERMs. If you have quality information in this area please message me!
Some foods that are plentiful in taurine include chicken (378mg/100g), tuna (332mg/100g), and slightly less but still large amounts in crab, shrimp, lamb, beef, eggs, and cheese. An equivalent dosage in humans for the longevity results found in mice may be somewhere in the range of 3-8g. This may seem like a large amount for a supplement, but if you were to eat 1lb of chicken that alone would contain ~1.7g. Acquiring notable amounts of taurine without supplementation can be difficult as a vegetarian and near-impossible as a vegan.
It’s also found in many energy drinks, sometimes in quantities as large as 0.5-1g, and there’s a bit of evidence that it may pair well to reduce the jittery aspect of caffeine in a way similar to l-theanine. It seems like 3g/day can be reasonably consumed safely, and I’d suspect that this carries at least up to 5=10g/day, if not much higher. I’m only moderately bullish (at most) on taurine improving human lifespan, especially if one begins with the assumption of a good diet, but I find it really interesting nonetheless.
Name: Semaglutide (now discontinued)
Dosage: 0.15-0.3mg (subcutaneous injection, once per week. may use in the future again)
Cost/day: $1-2 ($30-50/month, but reduced food intake can actually make this profitable to take!)
Description: Semaglutide [Wikipedia] is one of the most important inventions of the century. It is the weight loss drug known as Ozempic, Wegovy, or Rybelsus. There is so much literature on this drug (and it now has millions of prescriptions in the US) that I’m not going to go over it here, but the short version is that it not only works, but it works well, and seems to often have few or no negative side effects, and sometimes even positive side effects, from reduced cardiac events to many reports of improved willpower.
Obesity leads to millions of deaths, and now there is a cure for it which can actually be applied at-scale, even in the presence of relatively unrestrained markets with highly-addictive and caloric food. Semaglutide should receive a Nobel Prize.
Although it is known for being expensive when bought through FDA-approved mediums, it is possible to purchase it safely for significantly less as it is not a controlled substance. As I’m neither a doctor nor a lawyer, you should speak with your doctor if you’re interested in trying it out. If you have injectable (liquid) semaglutide, it should be refrigerated.
2024 update: I’ve discontinued semaglutide for two reasons, the first being that I no longer desire to lose more fat, and the second being that it reduces my hedonic baseline by a bit (that is, all of life is slightly less pleasurable). I may hop on it or try microdosing it in the future.
Name: Rapamycin
Dosage: 4-12mg (schedule and doses vary, taken at most once a week, many other factors)
Cody/day: $1-4
Information: Rapamycin is perhaps the most exciting substance for me in longevity right now. Rapamycin notably extends the lifespan of most organisms we have given it to thus far, but lacks proper research in humans aside from its use as an immunosuppressant. It’s a very popular drug to research in the area of longevity, and deserves a longer write-up than I’ve given it here. It’s also potentially quite dangerous and we have little data in humans (aside from those we give it to for organ transplants), so please don’t take it yourself (Jan 2021 update: mTOR Inhibitors Associated with Higher Cardiovascular Adverse Events ‐ A Large Population Database Analysis). Dosage for rapamycin is a bit tricky. There’s a lot of speculation involved, but it seems like many people converge onto something either like 6-8mg/week, or 8-15mg/2 weeks, perhaps with some breaks between.
2024 Update: Rapamycin blood tests are reasonably available – I currently shoot for around 25-45 ng/mL ~2 hours after initial ingestion as a reasonable baseline.
Out of all of the longevity agents I am interested in and/or take myself, it is likely to be the one that I have the highest hope for in humans. We have a decent understanding of the mechanism (compared to many other things, at least), it works very consistently and strongly in several other organisms, and the mechanism of action is strongly evolutionarily conserved. As for safety concerns, it seems like if taken in a low dosage and infrequently enough, the safety profile improves significantly and it may be a net-plus in many areas (this may be related to mtorc1 vs mtorc2 activation depending on the dosage and timing (it does have a pretty long half-life!), which also makes it seem like it can be taken without actually suppressing one’s immune system or causing some other undesirable effect categories).
Although I do know of many others that take rapamycin, I still don’t suggest it to anyone myself, firstly because I don’t offer medical advice of that nature regardless of my cost/benefit analysis (are there risks of potentially bad unknown side-effects with long-term usage? sure, but the risk of *not* taking longevity agents is also pretty large, and results in a much earlier likely death), and secondly because it is still likely to be higher risk than a lot of other simple things that I do often suggest to others, like glycine supplementation, which I see as close to zero risk. I’d hope that anyone that takes it themselves has blood panels done (if not much more) to ensure they’re not doing easily-observable harm to themselves as well. I’d like this section to be more comprehensive, but I’ll follow with some relevant pubmed papers for now:
Selegiline/L-deprenyl
is a MAO-B (and sometimes MAO-A) inhibitor sometimes used to help
treat Parkinson’s or depression which may be able to improve
lifespan in humans.
Dosage: 10mg/day for 5-10 days in a row, once or twice per year
Cost/day: $40
Epitalon is really interesting. A few concerns in humans and I don’t buy that the telomerase activation is the reason why it may have potential (if it does), but there’s a chance it passes EV calculations depending on how you do the math. I’ve tried it a few times and I’m uncertain if I’ll continue or not. More info here to be posted later.
Additional supplements I do not currently take
The above section concludes the actively-maintained list.
Under this I include a lot of links/notes from previous research, which is not comprehensive nor updated.
This section contains a list of supplements that I think might be worth taking, but that I currently don’t use. Substances in this section seem to be relatively safe, and I’m generally only not taking them because I have more doubts about their usefulness to me specifically.
Aspirin
Aspirin [Wikipedia]
is used for more than just treating temporary pain or fevers. As an
NSAID,
it reduces both acute and long-term inflammation, and may
also affect oxidant production, cytokine responses, and block
glycooxidation reactions. Consuming a low dose of aspirin daily
appears to lower the risk of CVD in higher-risk groups (generally
older
individuals with a relevant medical history), although appears to
have little
effect in otherwise
healthy individuals. The
risksof a
few cancers may be lowered
slightly by long-term
continualuse
of aspirin, although this is generally a minor effect, and
doesn’t seem to be the case for all types of cancer. Someorganizationssuggest
daily aspirin use in small doses for those in certain risk groups,
generally those that have already experienced a heart attack or
stroke.
Among aspirin’s more common adverse effects is an increased risk
of gastrointestinal bleeding, which is one of the reasons it’s not
suggested by most organizations for otherwise healthy individuals
with low CVD risk. Aspirin has increased
the average lifespan (although not the maximum lifespan) of mice
in some studies, but this is unlikely
to be the case in humans unless significantly more needs to be
taken, which would increase the probability of adverse effects
notably.
To summarize, it’s very likely that continual aspirin usage
reduces the risk of some types of cancer and moderately likely that
it can reduce the risk of CVD in some higher-risk groups. Although
side-effects are negligible for most individuals, it is difficult to
tell if aspirin is worth taking for healthy and young individuals.
It’s likely much more beneficial for the elderly or middle-aged, as
they’re at a much higher risk of cancers as well as CVD. As a
result of this, I don’t take aspirin regularly.
Cocoa Extract
Cocoa [Examine,
webmd,
Wikipedia]
is well-known as a major component of chocolate. Although the sugar
added to most modern chocolate definitely does not benefit one’s
health, cocoa itself has many bioactive substances with potential
benefits. Among the most notable is (-)-epicatechin, which can offer
improvements
in blood flow and a corresponding reduction
in blood pressure for many individuals. As usual, the most
notable improvements in blood pressure and cholesterol occurred in
individuals with pre-existing elevated levels. Some age-related
markers improve in mice when supplemented with (-)-epicatechin,
although no direct increase in lifespan has yet been noted.
Supplementation with some form of cocoa (supplemented or consumed as ultra-dark chocolate) may be beneficial for some individuals, although consuming too much sugar with cocoa would likely offset any positive effects. Quality cocoa extract is more expensive than many of the other supplements listed on this page, coming in at $1-2 day for a proper dosage.
Also, I’d love to purchase this and test it on myself for awhile to see if the effects can easily be measured.
CoQ10
CoQ10 [Examine,
webmd,
Wikipedia]
(Coenzyme Q10 / ubiquinone) is a substance found in meat and fish
that is primarily present in mitochondria and aids ATP production.
Although supplementation is likely safe, it’s difficult to find
convincing evidence that CoQ10 supplementation would be effective for
longevity. It may improve
lipid peroxidation, blood
flow and offer minor improvements in other areas, but in my
opinion doesn’t appear to stand out from most supplements, both
experimentally and theoretically.
Quercetin
Quercetin [Examine,
webmd,
Wikipedia] is a
flavanoid found in fruits and vegetables. As usual, eating the right
fruits and vegetables is good for you on its own, and may make
supplementation less beneficial, or completely irrelevant. I likely
get enough of this from my diet, although there may be benefits to
infrequent high-dose supplementation.
L-carnitine
L-carnitine [Examine,
webmd,
Wikipedia] is
an ammonium compound found in notable quantities in meat such as
beef. Supplementation sometimes appears to offer some decent results,
but I’ve determined that I like already get a sufficient amount
from my diet.
PQQ
PQQ [Examine,
Wikipedia]
is a redox cofactor found in human breast milk and some foods such as
kiwis. PQQ alters
indicators of inflammation and mitochondrial-related metabolism.
It’s likely very safe, the main reason I’m not currently taking
it is there’s very little evidence showing that it notably benefits
already-healthy young humans, and it costs a bit higher than most
supplements on this page.
Resveratrol
Resveratrol [Examine, webmd, Wikipedia] cannot go without being mentioned, as the extract from grapes that inspired the ‘red wine is great for you’ craze many years ago, it has been a constant source of speculative benefits and is still a very popular supplement in longevity communities. Although it hasn’t quite lived up to its initial hype, there’s still a lot of research on how it may be beneficial for longevity in one way or another. I’m personally not very into resveratrol and don’t see it as that interesting by itself. A summary is currently excluded here and you’re encouraged to read the above links if interested, but to be rather blunt, I think resveratrol is very likely approximately worthless, and is just yet another case study in now media hype in no way correlates with actual efficacy.
Sulforaphane
Sulforaphane [Examine, webmd, Wikipedia] is a compound found in vegetables such as broccoli and cabbages, with the best sources of it being broccoli sprouts and cauliflower sprouts. I’ve taken sulforaphane previously, but it will be difficult to know if it had a notable effect on me or not. I’m currently focusing more on my diet and have decided against taking sulforaphane. I’ve excluded a research summary in favor of the above links.
Some other supplements I am currently considering
Nicotinamide Mononucleotide (NMN) (Wikipedia): todo
Trimethylglycine [Exmine, Wikipedia] is a betaine amino-acid derivative found in some plants. It is notable for reliably reducing homocysteine levels in healthy subjects, sometimes by as much as 10%, and as much as 10-40% in unhealthy individuals. It appears that it might have a slightly negative effect in increasing, or preventing to some extent a decrease in, LDL, which is why I’m currently not taking it. It’s a nice molecule to be aware of and might deserve a spot in my stack at a later point, but as usual it would be nice to have more research available.
A lot of supplements have been excluded from this list, including many which are very interesting. Individuals who follow nootropic or longevity communities will definitely be curious why their favorite substance may have been excluded from this page, to which my answer is mostly that there’s too many substances for me to include all of them, so I did quite a bit of picking personal favorites. Even so, there’s likely many substances I’d like to include, but which I haven’t yet heard about or done enough research on. Feel free to message me on Twitter if you have any great suggestions here.
More interesting and potentially unsafe
substances
This section contains some brief notes and links on substances that appear to be a lot more ‘experimental’ than the above sections, but have some interesting potential. In some cases it’s impossible to find proper tests of safety, or even basic toxicity, in humans. Regardless, they’re all interesting chemicals, sometimes increasing the lifespan of organisms such as mice by large amounts. A lot of compounds have been excluded from this list as there are too many for me to list currently. The most interesting item of this list is currently rapamycin, by a large margin. Also see list of potential CRMs.
Allantoin
Allantoin
is a compound present in some cosmetics, toothpaste, shampoo,
lotions, and more, which has improved lifespan in C. elegans in
multiple studies.
Rejuvant®, a potential life-extending compound formulation with alpha-ketoglutarate and vitamins, conferred an average 8 year reduction in biological aging, after an average of 7 months of use, in the TruAge DNA methylation test: https://www.aging-us.com/article/203736/text
Astragalus Membranaceus
astragalus
membranaceus contains a compound called TA-65 that may
activate telomerase, extending the lengths of the shortest
telomeres in humans. This compound is lacking in notable research,
and much of what exists is clearly for-profit.
C60 is an interesting fullerene that has extended lifespan in some animals notable, but has little data on human consumption and safety. In an original study that gained quite a bit of attention, it was reported to ‘almost double’ the lifespan of rats. Now in 2021 the two most recent studies I see show that it did not extend lifespan, and that it only extended it by around 7%. There is less information on mechanism of action than we would want, but it is generally suggested to be related to free radicals.
There’s apparently quite a few people that have been taking this themselves, buying it from less-than-reputable Internet sources and hopefully not letting it be contaminated with light, as when exposed to light it degrades and becomes very dangerous to consume. This is certainly not something I plan to touch myself in with the current state of our knowledge on it, but it does seem like a very interesting chemical nonetheless.
Benzofuranylpropylaminopentane
Benzofuranylpropylaminopentane
is an unusual and understudied drug, in some ways similar to
selegiline noted above. It has prolonged lifespan to a minor extent,
such as 4% in mice.
GDF11 is also really interesting. Similar to Epitalon it’s obvious that the wikipedia article was authored by someone into longevity, but this is another thing I’m going to keep an eye on.
If you enjoyed this post or have corrections feel free to say hi on Twitter or any method on my about page